As we mentioned in our last article, after more than three decades of use, the International Classification of Diseases ICD-10 is giving way to its successor, ICD-11. It is worth continuing to analyse the new features and opportunities it offers.
1. Differences between ICD-10 and ICD-11 in terms of structure and content model
There are many significant differences between versions 10 and 11 of the ICD. The most relevant are:
- With regard to morbidity, the definition of primary condition has been revised and is now ‘the reason for admission, after assessment at the end of the stay (care)’. This definition is more precise and less prone to interpretation.
- Each code in ICD-11 includes a description of up to 100 words that mentions aspects that are always true about a disease or condition and that are necessary to understand the scope of the heading. This description helps to confirm that the selected code corresponds exactly to the patient’s disease or condition and improves coding accuracy.
- ICD-11 codes are alphanumeric and range from 1A00.00 to ZZ9Z.ZZ. Those beginning with ‘X’ indicate an extension code. These codes allow additional information to be added to the main code to describe aspects such as the severity of the disease, the external cause, or the extent of an injury.
- The key components of disease descriptions are included as different properties within the content model, providing greater precision, flexibility, and granularity to the coding. The main properties of the content model are:
- Title of the concept in the ICD.
- Hierarchy, type, and usage (parents, types, usage).
- Textual definitions: description (short); description (long).
- Index terms: inclusion terms and synonyms; exclusion terms.
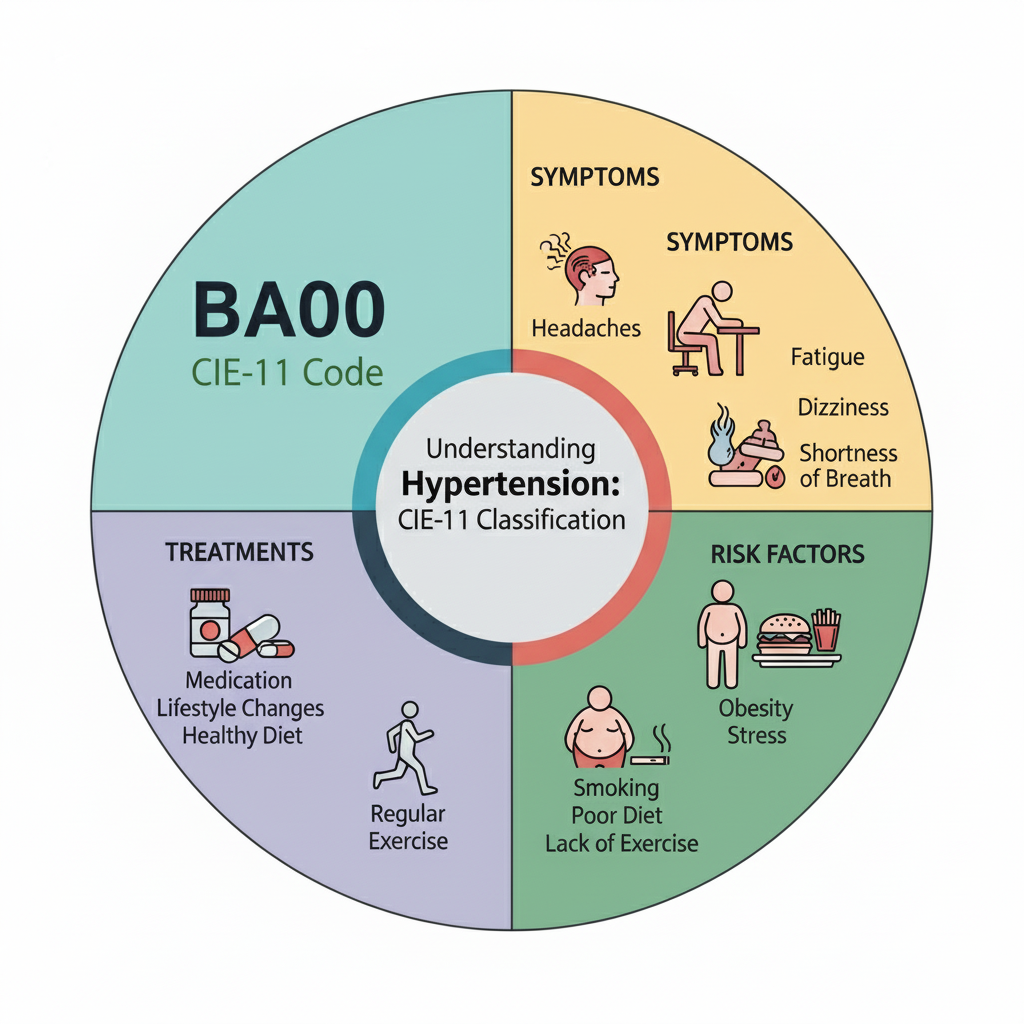
- Clinical descriptions: body systems; body parts or anatomical sites; manifestation properties (signs and symptoms and findings); causative properties; type of aetiology (infection and agents and injury or mechanism); risk factors; genomic characteristics; temporal properties; severity properties; functional properties; specific condition properties; treatment properties; diagnostic criteria.
2. Applications
A. Complete electronic format: for the first time, the ICD is available entirely in electronic format and can be browsed online. It currently provides access to 17,000 diagnostic categories, with over 100,000 indexed medical diagnostic terms.
B. Advanced search: the indexed search algorithm interprets over 1.6 million terms. Doctors can search for diagnoses using natural language or their preferred terminology, and the system automatically links it to the correct technical code. This means doctors do not need to memorise codes.
C. Integration into electronic health records: Its integration into existing digital record systems combines recording with coding, allowing coding to be a natural part of medical record-keeping (fewer steps, fewer errors). This ensures compliance with specifications by users.
D. Expandable ontological core: the ontological core of ICD-11 can be easily expanded to accommodate new terms, synonyms, and concepts, or to improve user guidance, in all language versions.
E. Browser and API: ICD-11 has a web browser that allows users to retrieve concepts by searching for terms by diagnosis, anatomy, or any other element of the content model. It also has an API for integration into healthcare software (medical records, health apps, billing systems, etc.).
3. ICD-11 semantics
One of the greatest advantages of ICD-11 is the removal of the coding barrier for healthcare professionals:
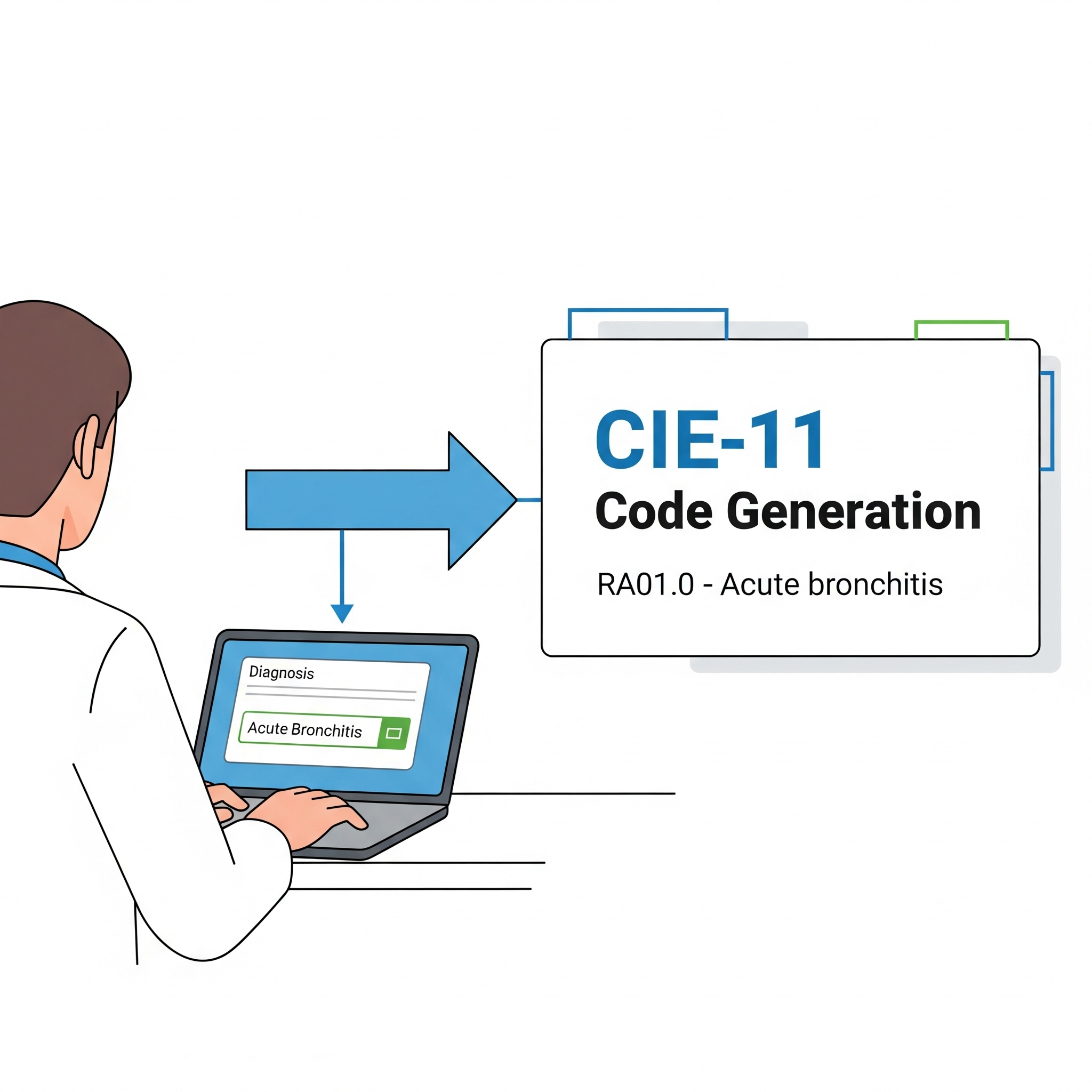
A. With this new version, it is now possible to optimise the classification process without the need for a ‘coder’, as semantic analysis and natural language processing allow doctors themselves to categorise diagnoses when writing their clinical assessments, without the need for codes and based on the system’s suggestions.
B. In a semantic environment, codes lose relevance and are only used internally and for technical design purposes, but they can be transparent to the end user.
C. A clinical HIS integrated with ICD-11 will semantically search for the terms used by the professional and suggest the diagnoses that most closely match what is being described.
D. It can even be used as a batch (offline) system, analysing medical descriptions and texts (at a later time) to automatically suggest related base codes (diagnoses) and confirm them in a supervised manner.
E. Electronic documentation shall follow the principle of lossless information collection at source. Best practices include information on:
- A text field that collects the clinical term with the exact wording reported by the healthcare provider.
- A data field that retains the identifier (URI) of the selected entity from ICD-11 (index, code title, or other element) that represents the closest match for that text (if present).
- A data field for the corresponding ICD-11 code.
4. Summary
With ICD-11, thanks to its design based on ontological and semantic models, and digital tools such as APIs and web services, clinical coding is completely changing. Classification is now integrated directly into health information systems (HIS), eliminating the need for a specialised coder. It is the clinician themselves who automatically generates the corresponding code while recording clinical information: they write the diagnosis in natural language and the system translates it into the official code, without the need to memorise it or rely on subsequent interpretations.