1. Introduction
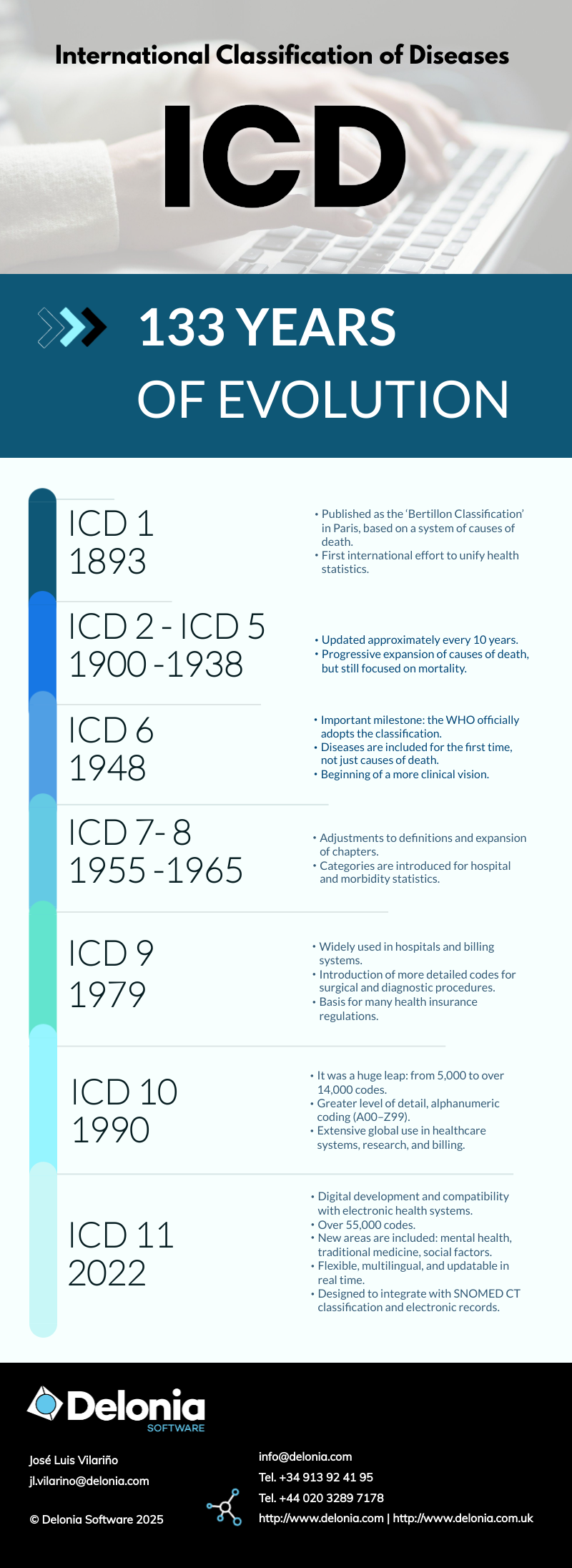
Since 1 January, 2022, the new International Classification of Diseases, ICD-11 (International Statistical Classification of Diseases and Related Health Problems), has been in force. This new proposal differs greatly and profoundly from previous versions and opens up the possibility of multiple applications in the world of Digital Health.
To fully understand how to use this tool, let us recall a few concepts:
- The healthcare professional responsible for treatment is also responsible for documenting the patient’s health conditions. This information should be organised systematically using standard recording methods.
- A properly completed medical record is essential for good patient management. It is also an essential prerequisite for creating a valid coded record of patient diagnoses.
- When there is a good written record of the patient’s conditions, the satisfactory coding of this information in the ICD and associated classifications produces a valuable source of epidemiological and statistical data on morbidity and other health problems.
- A minimum set of data suitable for international comparison would include age, sex, and primary diagnosis or condition (i.e., the reason for care or admission after final assessment).

This new version 11 adds much more information, incorporates an ontology-based design, and integrates CIF and CIIS methodologies into a common platform. In this regard, it can be used not only in clinical practice, but also in the administrative and insurance fields.
2. Fundamentals of the new ICD-11
2.1 Principles of coding in ICD-11
The basic coding of the model is based on:
- Base code: ICD-11 codes are alphanumeric and cover the range from 1A00.00 to ZZ9Z.ZZ. They are called base codes.
- Extension code: There are extension codes (prefix X) that can be used to add more information to a base code. These are groups of codes used to provide further details, for example, anatomy, agent, and histopathology, among others.
- Post-coordinated code: Post-coordination is a notable new feature of ICD-11 that allows multiple main codes or base codes to be combined to describe a diagnosis in greater detail and precision. Extension codes can also be added to a base code to include additional information (such as location, severity, cause, etc.). In this way, the classification can address a large number of clinical concepts.
- Pre-coordinated code: There are base codes that contain all the relevant information in a pre-combined form. A pre-coordinated code is a unique and complete code that encompasses all the information for a diagnosis or clinical situation, without the need to combine it with other codes. These pre-coordinated base codes represent very common or clinically important diagnoses. They are an advantage for professionals, who do not have to construct the code piece by piece, as the system provides them with one that is ready to use.
- Cluster: Another important concept is that of cluster in ICD-11, which refers to the combination of several codes that are interpreted as a single composite clinical diagnosis, reflecting both the cause (e.g. diabetes) and the manifestation (e.g. neuropathy). It is used when there is a clear causal relationship between diagnoses (cause → manifestation).
2.2 Key aspects of ICD-11
- Functioning and assessment Whodas 2.0 and the ICF: For the first time, ICD-11 includes a specific section on people’s “functioning”, aligned with the WHO’s ICF (International Classification of Functioning, Disability and Health). This means that, in addition to stating what disease a patient has, it is now possible to code how that disease impacts their ability to live and work. Furthermore, the WHODAS 2.0 methodology is considered an assessment tool.
- Symptoms and findings: There is a section for clinical findings that is used to classify general symptoms and clinical findings without a definitive diagnosis or when the information to be recorded is precisely the sign or symptom itself. For example, the chest pain code can be used if it is not yet known whether it is a heart attack or muscle spasms.
- After-effects and residual conditions: Conditions documented as after-effects (late effects) will normally be classified using post-coordination as appropriate. In addition, when the patient no longer has the original disease, the healthcare professional should code both the residual condition (after-effect) and its origin, along with a clear indication that the original disease is no longer active.
- Injuries and external causes: ICD-11 requires two dimensions to be coded for injuries and external causes: 1) The injury itself. 2) The circumstance that caused it. External cause of morbidity or mortality (chap. 23, as a modifier). It is assigned as an additional code and is coordinated with the nature of the injury, as it can be considered a modifier.
- Personal and family history: ICD-11 allows personal and family history to be recorded as part of official clinical information, something that was previously left out or collected in a scattered manner.
- Codes for conditions ruled out: ICD-11 includes a series of codes that can be used to describe care in which a suspected condition has been ‘ruled out’. In other words, the reason for the consultation is recorded and a clinical record is made stating that it was evaluated and ruled out. These codes appear in Chapter 24 as children or descendants of QA02 (‘Ruled-out conditions’).
2.3 Levels of descriptive information
There are four levels of descriptive information in the ICD-11 content model:
o Fully specified term – This is an unambiguous title that does not assume context.
o Short description – This is a short text (maximum 100 words) from the organisation that includes only what is always true about that disease or condition.
o Additional information – This is a text field that is not mandatory, but may contain additional information or characteristics of the diseases. This field provides context (epidemiology, causative agents, common characteristics).
o Clinical or diagnostic criteria – Contains one or more scenarios or clinical characteristics sufficient to diagnose the condition.
In summary, ICD-11 offers a more accurate, flexible and clinically focused view, reflecting not only current diseases, but also their context, sequelae and real impact on patients’ lives.
In our next article on ICD-11, we will analyse in detail the differences with ICD-10, both in its structure and content model, explore its main applications, and see how it opens up new possibilities thanks to advanced semantics and the use of natural language.